The curious case of oesophageal cancer
Cases of oesophageal cancer have an unusual pattern across the world. Some very specific regions can have a large numbers of cases but neighbouring regions have very few people affected. Here, Dariush Nesheli from IARC explains how researchers are working to uncover the reasons why this happens.
Mutational signatures can be thought of as signs that hint of the harmful events that occurred to DNA long ago, similar to how fossils are an imprint of a long-lost animal. For this reason, they can provide clues about the possible processes that can lead to cancer. Epidemiologists and molecular biologists measure changes to DNA, known as mutations, to see if these changes can be linked to causes of cancer such as smoking. This will help to discover and confirm potential cancer causes and understand the mechanisms that underlie why we get cancer.
In collaboration with Wellcome Sanger Institute, the International Agency for Research on Cancer (IARC) is part of the £20 million “Mutographs of Cancer” project. On this project, we are studying mutational signatures in 5000 cancer patients. Of these, 2000 people will be donating samples of oesophageal cancer.
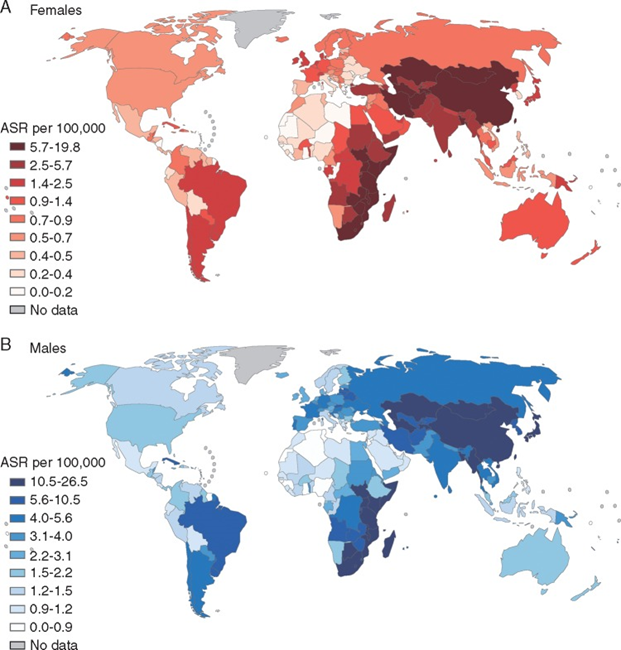
Cases of oesophageal squamous cell carcinoma for women (top) and men (below). Source: GLOBOCAN 2012.
The oesophagus and oesophageal cancer
The oesophagus is a 25 cm pipe that transfers liquids and foods from the mouth to the stomach. There are two different types of oesophageal cancer. The most common is squamous cell carcinoma (OSCC). This is where the cancer begins in the cells that line the oesophagus. OSCC accounts for 80% of oesophageal cancer cases worldwide. The less common type, oesophageal adenocarcinoma, comes from the glands in the oesophagus. Cases of oesophageal adenocarcinoma have been increasing in western countries in recent years. The symptoms of both types of oesophageal cancer are well known: to begin with, there is difficulty in swallowing solids and then liquids, and the oesophagus will end up being totally blocked by the tumor. Due to the way the tumor grows, when the first symptoms appear, it is often too late to cure the cancer as the condition has already progressed too far.
‘Hot zones’ for oesophageal cancer
Based on early studies in high risk areas of Brittany and Normandy in France, oesophageal cancer was first thought to be something that mostly affected men. About 90% of cases could be linked to drinking large amounts of alcohol and tobacco smoking. Between 1967 and 1969, IARC introduced regional cancer registries in the Caspian littoral area of Iran, as there were also reports of a very high number of cases of oesophageal cancer in that region. The initial findings of these registries resulted in a new understanding of the mechanisms and causes of OSCC in these particular areas:
- The rates of OSCC in women were equal or even exceeded those in men
- Drinking large amounts of alcohol and smoking cigarettes did not explain the high occurrence of OSCC
- There was a striking difference in cases of OSCC between communities that were separated by as little as 100 km (60 miles). This suggests there may be ‘hot zones’ for OSCC, where something in the local area is causing the condition
Further reports and emerging data have highlighted several other ‘hot zones’ in Eastern South America, Eastern Africa (“African Cancer Corridor”), and Central Asia (“Asian Cancer Belt”).
To address the causes of these patterns, several IARC collaborative studies were conducted: in the 1970s in Iran (Gonbad); in the early 1980s, when a preventive trial was conducted in China (Henan) to investigate possible effect of supplementing food with vitamins and minerals on OSCC risk. Between 2002 and 2004 studies took place in the Golestan province of Iran. The Golestan study used expertise from IARC to create a large-scale tissue bank of donated cancer tissue, allowing for large amounts of data to be collected and analysed. Furthermore, there has been a collaborative study with several countries in the “African Cancer Corridor”.
Risk factors for oesophageal cancer

Maté tea (Credit: Jorge Alfonso Hernández, Wikimedia commons)
It has become clear from the research to date, that there may be many different causes for OSCC that vary by region. Emerging data suggests some risk factors could include hot drinks (scalding hot tea, hot Maté), opioids, poor dental hygiene, indoor air pollution from burning solid fuel in inefficient stoves, high levels of chemicals called polycyclic aromatic hydrocarbons and a diet low in fruit and vegetables.
The Mutographs project and oesophageal cancer
One of the aims of the Mutographs project is to explore the differences between the reported causes of OSCC across continents. Taking advantage of the well-established IARC collaborations across the globe, a large number of samples will be available from populations where the cases of this cancer are high, and other regions where there aren’t many cases. The huge variation in cases in different places, in addition to access to a huge number of samples presents new and improved opportunities to investigate the mechanism(s) associated with both genetic and environmental risk factors among high, intermediate, and low risk areas for OSCC.
- Read more about the latest findings on hot tea and oesophageal cancer on the Sanger Institute blog.